

Knowledge, Attitudes and Practices COVID-19 Dashboard
An interactive visualization designed for policymakers and public health officials who rely on data and informed decision-making to craft public health messages and campaigns related to COVID-19.

An interactive visualization designed for policymakers and public health officials who rely on data and informed decision-making to craft public health messages and campaigns related to COVID-19.
This is a short technical brief with important steps and resources on how country programs can track and address rumors around COVID-19. The guide includes a number of resources and links while also sharing nuggets from global, collective thinking around rumors.

The COVID-19 Communication Network is a reliable site for social and behavior change (SBC) professionals, and other responders in need, to access and share high quality communication materials, tools and resources from global partners to address the COVID-19/Coronavirus pandemic.

Springboard is an online community of social and behavior change (SBC) professionals who are passionate about making a difference in the world. Members seek access to experts, the latest theories and tools and the most stimulating discussions and educational opportunities, in order to advance their own knowledge and skills.
This document includes important considerations and resources to support country programs in creating a functional rumor management system, enabling two-way communication with affected communities.
This technical brief details the steps and considerations programs can take to develop an overarching social media strategy to disseminate COVID-19 messages and combat misinformation. This document also provides a list of relevant tools and resources for implementation.
Integrating gender into the COVID-19 risk communication and community engagement (RCCE) response demands consideration of how gender norms and roles, as well as inequitable power dynamics and decision-making, influence people’s experiences and needs at all stages. This technical brief provides practical recommendations to integrate gender across the six pillars of the RCCE response.

The Compass is a curated collection of social and behavior change (SBC) resources. The collection offers the highest quality “how-to” tools and packages of materials from SBC projects. Each item in the Compass is vetted to ensure it was developed via a strategic process and had documented success in the field.
This website, ipc.unicef.org, is part of a global package of tools and resources designed to support frontline health workers in their immunization work, with a focus on improving their capacity to effectively use IPC to address barriers to immunization uptake and completion. The primary audience for the interpersonal communication for immunization (IPC/I) package is frontline health workers who provide immunization services.

The Malaria Behavior Survey is a cross-sectional household survey of malaria-related behaviors and the factors that drive or inhibit them. The survey uses a theory-driven and standardized methodology to produce data to inform malaria social and behavior change interventions.

Global Health: Science and Practice (GHSP) is a no-fee, open access, peer-reviewed online journal intended to be a resource for public health professionals who design, implement, manage, evaluate, and otherwise support health programs in low- and middle-income countries.
This document is a resource for individuals and coalitions seeking to increase advocacy for the inclusion of vasectomy in family planning and reproductive health (FP/RH) investments, programming, and national strategies.
This framework is a resource for actors seeking to advocate with coordinating bodies, donors, and low-and middle-income country (LMIC) decision-makers to enable comprehensive method choice by expanding access to vasectomy. This resource is not meant to help health programs design messages to increase social support or generate demand for vasectomy at the user-level.
Breakthrough ACTION worked with partners from 24 donor and implementing organizations to develop and validate a global shared agenda for social and behavior change (SBC) in family planning. The Shared Agenda identifies five strategic priorities for SBC in family planning across three areas where increased investment, coordination, and collaboration are most needed.
Advocating for social and behavior change approaches? Understand the factors that influence whether a stakeholder invests in or supports social and behavior change. Take our short quiz and receive guidance on how to lead a successful conversation.
Nous simplifions la promotion d’approches de CSC dans les programmes de planification familiale. Répondez à notre bref questionnaire, puis nous vous fournirons des conseils sur la façon de mener une conversation avec succès.

The Provider Behavior Ecosystem Map is a thinking tool designed to help you understand and consider diverse factors that influence facility-based provider behavior, and how they interact with one another, as you design or adjust your provider behavior change initiatives.

This report explores formative research findings and specific behavioral economics mechanisms that are relevant to the ways in which FP/RH professionals seek out and share information. The report recommends how organizations and programs can address barriers and opportunities, and explains the implications of these findings for knowledge management within the FP/RH community.

Knowledge SUCCESS hosted a series of four regional workshops in mid 2020 with FP/RH professionals from Anglophone Africa, Francophone Africa, Asia, and the United States. Using a design thinking approach, participants identified common barriers and behaviors that are limiting the flow of family planning knowledge between programs, countries, and regions — and opportunities to transform the way our FP/RH community approaches knowledge management. This report analyzes trends and findings across all four workshops by each step in the design thinking process.
This collection of resources is for family planning program planners, designers, and implementers who want to understand and measure social norms and social norms shifting interventions and incorporate them into their work.
This collection of essential resources is designed to help program planners, designers, and implementers in a variety of sectors (such as environmental conservation, resilience, food security, and economic development) understand and explore elements of PHE programs so that they can incorporate this approach into their work.
Une collection organisée par Knowledge SUCCESS et Family Planning 2020 pour les professionnels de la planification familiale qui conçoivent et mettent en œuvre des programmes dans les pays francophones à faibles et moyens revenus.

The Knowledge Management Index (KM Index) is an assessment tool, developed by The Knowledge for Health (K4Health) Project, to examine an organization or project’s use of KM practices, identify opportunities for improvement and, map out an action plan to strengthen the KM capacity.
The Global Health Knowledge Collaborative (GHKC) Knowledge Management (KM) Indicator Library offers a set of tools and comprehensive guidance to anyone designing KM activities and measuring KM approaches, in particular those who working in the field of global health and development.
The Building Better Programs guide is part of the Knowledge for Health Project’s Knowledge Management Collection, a family of resources designed to help global health professionals understand, use, and train others on knowledge management (KM) approaches, tools, and techniques.
The Pocket Guide provides a basic overview of the Knowledge Management Road Map and serves as a quick reference on key steps for applying the Road Map to global health programs.
CCP-led Breakthrough ACTION produced a real-time rumor tracking system design and implementation guide for humanitarian and public health organizations as well as national governments seeking to document rumors in a systematic and dynamic fashion. The guide lays out an application of this approach using the District Health Information System 2 (DHIS2) open source software platform, including an overview of a pre-configured metadata package that can be installed on a new DHIS2 system or imported to an existing system.
People-Planet Connection is a Knowledge SUCCESS-designed website dedicated to collaboration on population, health and the environment (PHE), just as people around the world celebrate restoring the planet and environmental protection. It is envisioned as a space for development professionals around the globe to gather to
FP insight is the first resource discovery and curation tool built by and for family planning and reproductive health (FP/RH) professionals.
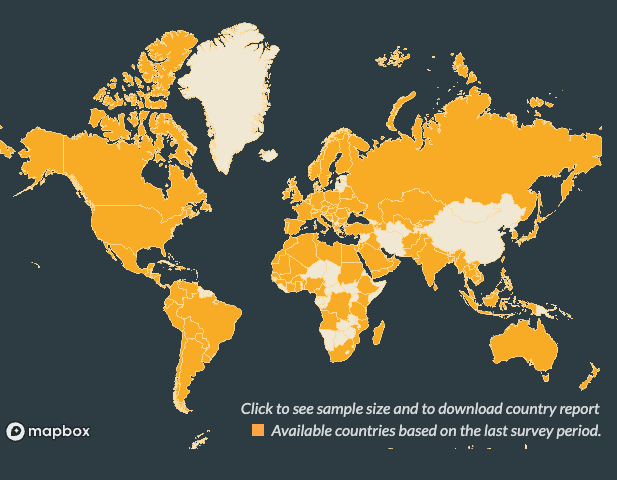
The COVID Behaviors dashboard presents data from a global survey of knowledge, attitudes and practices around COVID-19. Insights and analyses on how to use the data were written by researchers and social and behavior change communication experts at Johns Hopkins CCP in collaboration with WHO’s Global Outbreak Alert and Response Network (GOARN).

In addition to the broader toll it takes on mental and physical health, intimate partner violence significantly impacts family planning uptake and outcomes. This Breakthrough ACTION tool summarizes the findings of an expert consultation on using SBC to address this intimate partner violence.

The Knowledge Management Training Package for Global Health Programs is an online training resource with numerous ready-to-use training modules for KM trainers and health program managers. It covers topics ranging from how to apply KM in global health to storytelling, visual content, peer assists, and after-action reviews with the goal of strengthening the capacity of the global health workforce to manage and share critical knowledge needed to deliver results.

The Social and Behavior Change Flow Chart is CCP’s design process for social and behavior change activities to address health or development challenges. The SBC Flow Chart comprises three phases, Define, Design and Test, and Apply. This integrated approach draws on design, behavioral science, community engagement, market research and communication, and brings together the strengths of each discipline, methodology and technique to create new opportunities for innovative SBC solutions.

Incorporate new social and behavior change approaches into your work with these learning opportunities.
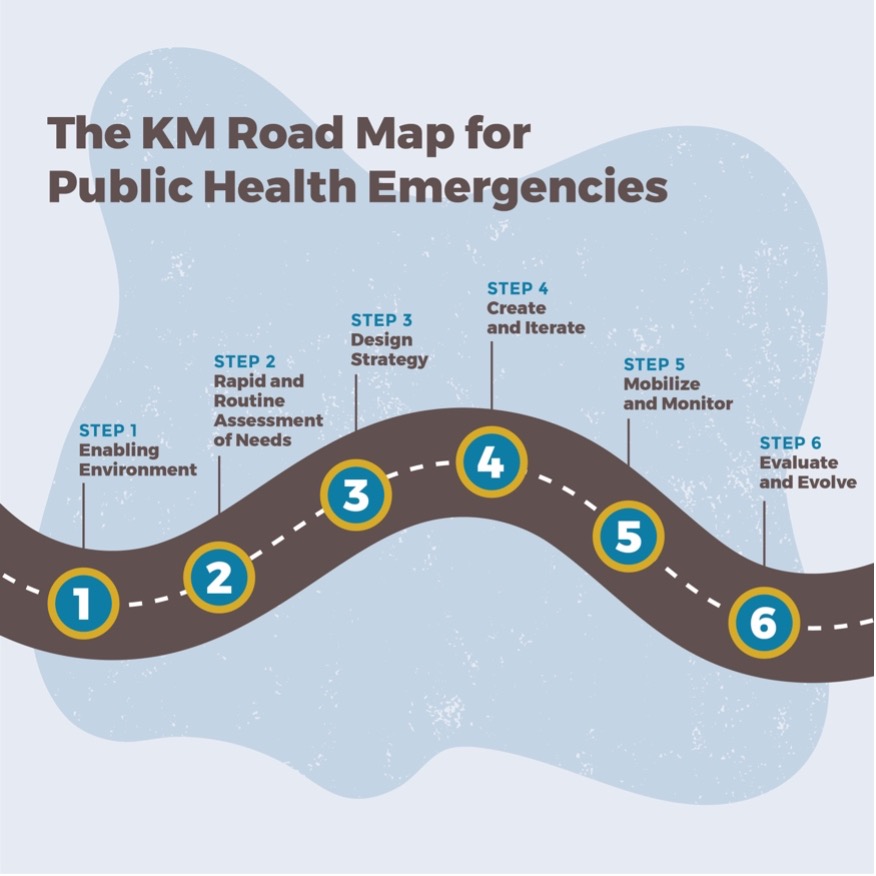
This KM Road Map for Public Health Emergencies provides an overview of how to implement KM during a public health emergency, such as an infectious disease outbreak. It outlines a step-by-step process that implementing partners, public health professionals, and donors can adapt to their contexts.
Receive the latest news and updates, tools, events and job postings in your inbox every month